This month marks the 49th year since I was diagnosed as a Type 1 diabetic. Back in 1970 they actually hospitalized me 10 days to stabilize my sugar levels and to educate me and my parents about this new routine of daily injections.
I do not remember my parents worrying about the cost of medication. I have no idea what insulin cost then, but I would guess it was covered under the health care plan my father earned as a US government employee.
Those three vials in the photo above are a one months supply for me now, and the range of prices one might pay for that depending on where in the world you live, and if in the USA, which flavor of health insurance you might have varies over orders of magnitude. For some people it might be $50, for others over $1000. How is that even possible? What kind of system produces this disparity?
If I am looking at my old checkbook entries correctly, in 2005 with employer health coverage this supply might have cost me $25. Later, under the ACA healthcare plans I paid for, accounting for deductibles, in 2013 those three bottles would have been $120.
Read these numbers and explain to me how this is possible:
In recent years, insulin prices have skyrocketed, according to figures compiled by the Senate Finance Committee, which is investigating possible price gouging in the industry.
Between 2001 and 2005, Eli Lilly’s Humalog increased from $35 to $234, a 585 percent increase, the Senate panel found.Americans are dying because they can’t afford their insulin. That’s now a 2020 campaign issue. (Think Progress)
Novo Nordisk’s Novolog rose from $289 in 2013 to to $540 in 2019, an 87 percent increase. Sanofi’s Lantus, meanwhile, increased in price from $244 to $431 between 2013 and 2019, an approximately 77 percent increase.
The 2016 T1International Insulin & Diabetes Supply Survey clearly showed that the costs of insulin in the US was double, quadruple, even more the price for the same medication in other countries.
Meanwhile, people are dying because they cannot afford these unevenly distributed high costs of life critical medications.
Is the price based on cost to produce? The article on Beyond Type 1 How Much Does it Cost to Produce Insulin caught my attention. Summarizing a research study by Imperial College London, the Harvard TH Chan School of Public Health, and Liverpool University, it suggests a year’s supply sound be something under US$75. Note that the full research paper, published under Creative Commons is amazingly available for free to view.
Then there is this visual:
Almost a year ago, I decided to send an email message to my quote/unquote Representative, Paul Gosar, asking him, as a medical practitioner and self appointed advocate of health issues, what he could do about breaking the insulin monopoly. I included the reports above as references.
In January 2018, response arrived from a staff member in Gosars office that hardly answered the question.
Thank you for contacting the Office of Congressman Paul Gosar on the issue of Insulin and the rapid price increase. It’s true, drugs like Insulin have risen at a meteoric pace that is troubling to say the least. You referred to the monopoly in the insulin industry being a cause and of course, 3 companies is by no means a comparatively competitive marketplace but this is not the main source of the rise in prices. Like many bad things in healthcare, excessive government intervention is the culprit. Innovation is the key to refining and improving any industry but like government often times does, it stifles innovation. Drug prices are no different. Any drug that goes from an idea to a reality needs to go through a long, arduous process. This is done mainly because of the stringent FDA regulations to get a drug approved and produced for the market. Since Insulin is a biologic drug, the process is even longer than other types of drugs. During the Trump Administration, the FDA approved a record number of generic drugs in order to foster competition in various health industries. In order to lower all drug prices, this activity needs to continue and be ramped up if at all possible. There are so many steps to get a drug approved that monopolies often times form and it’s because the lobbyists of big drug companies can create these barriers that their company can easily jump but smaller companies cannot.
Response from Representative Paul Gosar, emphasis added by me
So the culprit here is “government intervention”? What even does that vague reference mean? It’s more or less the “bogeyman”.
Actually there is a better explanation on how insulin pricing works in the US (again from Beyond Type 1) where one learns of the entities known as PBMs or Pharmacy Benefits Managers.
Pharmacy benefit managers, or PBMs, are the player that is hidden in plain sight. The three largest PBMs are Express Scripts, CVS Caremark and OptumRX. PBMs are third-party intermediaries who negotiate prices between pharmaceutical companies and insurance companies. However, the lines between insurance companies and PBMs are becoming increasingly blurred — OptumRx is owned by United Healthcare, Cigna recently merged with Express Scripts, and CVS Health acquired Aetna.
How Insulin Pricing Works in the US
PBMs’ stated goal is to reduce costs from pharmaceuticals for the insurance companies while improving health outcomes for the members of the insurance plans. They participate in the rebate system and take a share of the profits from prescriptions that are sold to members of the insurance plans. This group is often invisible to consumers and can drive up the costs of prescriptions without consumer awareness.
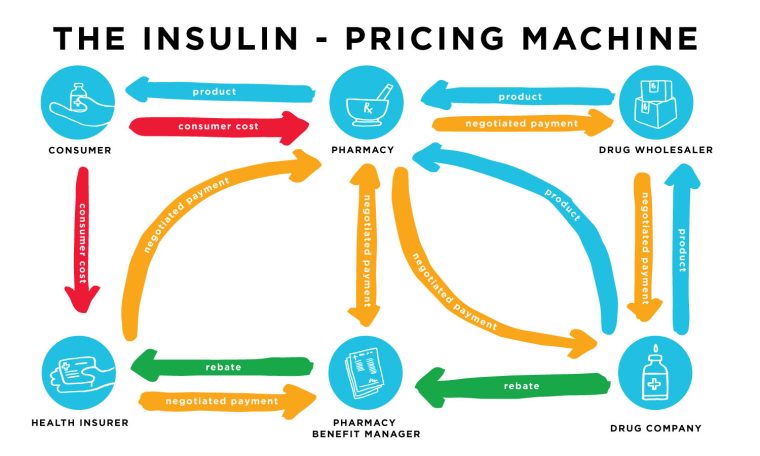
There are 6 blue circle entities in this diagram; all of them except the consumer have a slice of the profit pie.
Rebates between manufacturers and PBMs are hardly the end of the story. Let’s explore this web a bit further. Insulin arrives at the pharmacy either directly from the pharmaceutical company or through a prescription drug wholesaler. There are negotiated payments from the wholesaler to the drug company, from the pharmacy to the wholesaler or drug company, from the insurance company to the pharmacy, from the insurance company to the PBM, and between the pharmacy and the PBM. Then there are the rebates the drug companies give to the PBM and the PBM gives a portion of that rebate to the insurance company. This all changes the cost from the time the insulin leaves the manufacturer until it reaches the customer at a retail pharmacy.
Customers pay at the pharmacy when they receive their medications, and if they have health insurance, they are responsible for the co-payment and premiums. Depending on the insurance plan, prescription drug costs may or may not contribute toward the deductible, but they do count toward the out-of-pocket limit. These plans and rates are not standardized, so people who need insulin end up paying a wide range of prices when they pick up their medication at the pharmacy.How Insulin Pricing Works in the US
The consumer cost is affected by all of these behind-the-scenes negotiations and rebates because there are five parties making money from a single transaction.
No, Representative Gosar, it is definitely not government invention causing the cost of insulin to increase at rates beyond almost anything else.
The proof is across the border.
I moved to Canada in May 2018. They do not just toss free healthcare your way (it took until March 2019 when I got my permanent resident status). I arrived with a 3 month supply (at the $120 per month cost), and as I relied on my ACA coverage, I was able to order my supplies sent to my Arizona address, where a friend was able to mail to me here (the costs now had a shipping topped on top). I was under the impression I could only do this once, but my friend located a regulation that said for personal use, I could get another 3 month supply sent (checked with calls to Canada Customs). It was cumbersome, but at least I could get my insulin.
Then, almost on a whim, I called a local pharmacy to ask if insulin could be bought over the counter, without a health card. The answer was yes! “Do I need a prescription?” (thinking I would need to see a doctor). “No, pharmacists can write these).
The cost per bottle of insulin here was CA$35 (US$27).

Way to Go Canada flickr photo by cogdogblog shared into the public domain using Creative Commons Public Domain Dedication (CC0)
The very same bottle, same stuff inside, same packaging outside, without insurance, that cost 10 times as much in the US can be purchased over the counter in Canada! How can the same same item, the same costs to produce, vary so much? (see the five hands in the profit pie above).
At least there is finally some pressure from the Congressional Diabetes Caucus on the big three companies that form the insulin cartel, who are making some feigned moves towards price changes. The Senate is applying pressure and Colorado is too.
There is no way that anyone anywhere should not be able to obtain life necessary medication like insulin because of a cost machine.

2014/365/307 Eight Bottles flickr photo by cogdogblog shared under a Creative Commons (BY) license
The act of “evergreening” by the insulin cartel allows them to infinitely prolong patents and completely squash the development of generic brands of insulin that would be competitively priced.
So a positive ray of light here, working from the other end, is an effort towards open sourcing insulin production:
This is more in the spirit of the (Canadian) medical team that first isolated insulin. They put their patent into the public domain, never intending it to be a billion dollar profit industry.
Stuff I Remembered Later…
Featured Image:

A Month of Life Juice flickr photo by cogdogblog shared into the public domain using Creative Commons Public Domain Dedication (CC0)

Alan thanks for writing this. It gives me hope some countries are still halfway rational.
I can’t help but think that whole episode with Martin Shkreli (https://en.wikipedia.org/wiki/Martin_Shkreli) emboldened more than a few dopes and bozos in the pharmaceutical industry to “try” something in the pricing arena and see what would happen with regulators. And true to form nobody really clamped down or stated categorically this would not be tolerated. So the game was afoot to see how much the pricing could be gamed and not be prosecuted as criminally illegal.
Furthermore, I will seriously consider giving up might rights as U.S. citizen to gain access to healthcare, prescriptions, the whole lot if I have to. No doubt
Bernie Sanders agrees with you: https://www.theguardian.com/us-news/2019/jul/28/bernie-sanders-americans-canada-insulin-bus-caravan
Bernie is on it! I keep remembering more links to add, like https://www.affordableinsulinnow.org/